Co-authored with Peter Hoffman
First published 23 March 2026
Explaining Infection Risk from Theatre Headwear: A Microbiologist and Guideline Methodologist Perspective
I am not a clinician but a guideline methodology expert; you can read my full disclaimer here.
I feel very fortunate to have had the opportunity to work with Peter Hoffman on guideline development over the years. His ability to cut through assumptions and focus on underlying mechanisms has always been fascinating, and I have learnt a great deal from listening to his perspective.
This post arose from a recent discussion about a study examining contamination of different types of theatre headwear. The findings have been interpreted by some as having implications for surgical site infections (SSIs). However, the key issue is not the study itself, but how its findings are being used.
Please note that this is not a criticism of the study. It is a question of relevance: Does measuring contamination of headwear meaningfully inform our understanding of SSI risk?
Currently, no established link exists between theatre cap contamination and SSIs. Yet, the discussion appears to move quickly from “contamination was detected” to “this may increase infection risk.” This leap in reasoning is where the real problem lies.
To explore this properly, it is helpful to consider two complementary perspectives. This is why I invited Peter to contribute to this post, and I am very grateful that he agreed. I hope you find it valuable to read both a microbiologist’s view of contamination and transmission, and a guideline methodologist’s perspective on how evidence should inform practice.
Peter’s perspective: the microbiologist’s view
Context: Operating theatres are not sterile. They should be reasonably clean (a poorly definable concept), until you put the operating team and patient in them. This introduces billions of microbes. Infection prevention is about ensuring that as few as possible of these microbes get into the surgical wound. The core concept here is the “sterile field” – a functional unit within the operating theatre that separates out truly sterile surfaces (e.g. the scrub team’s gloves, sterile gowns, the instruments, sterile drapes etc.) and these can have contact with themselves and the surgical wound but no contact with surfaces outside this defined area.
There’s an additional factor that needs consideration – the air. The air supplied to an operating theatre has passed through fine filters. It’s not sterile, but very low contamination. This is where the people in the theatre and their billions of microbes mess things up. Skin is a body organ that is continually renewing itself; the basal layer of cells produces new cells (“squames”) that are pushed upwards. As they reach the top, they die and dry (think microscopic cornflakes) and are released from the very top layer into the air. (The light grey dust that accumulates on bookshelves is mainly settled skin squames from people who have been in that room). Some of these will carry microcolonies of the bacteria and yeasts that grow on the skin and the ducts, glands and follicles within. In the context of an operating theatre, the requirement is to prevent these from settling out not only into the surgical wound but also onto the instruments that will have contact with the surgical wound. This is achieved by introducing vast amounts of clean air into the theatre and encouraging it to then flow out of the theatre into adjacent less clean rooms, taking these contaminants with it. Whilst well designed full body exhaust suits and integral helmets worn by the surgical team may reduce dispersion into the air, normal theatre wear does not.
So this aspect of infection prevention does not focus on elimination of microbes, but on interrupting identified routes of microbial transmission within an inevitably contaminated greater environment. Yes, it’s nice if the environment isn’t too mucky but that, of itself, isn’t going to solve your problems.
All this is a preamble to what Aggie has asked me to comment on: theatre headwear and contamination recoverable from it. I think that hair has maybe too high a profile in the perceptions of infection prevention in theatres. Hair is contaminated, but each hair is a very self-contained unit. It is not going to release fragments equivalent to skin squames and microbes are not going to spontaneously detach themselves into the air. If a hair, along with all the microbes on it, falls onto exposed instruments or into the surgical wound, that is a very significant event. The function of headwear is to stop that happening; it is not to prevent airborne dispersion. Headwear will inevitably be contaminated by the wearer, both by contact with their contaminated hair and by trapping squames released from the scalp, ears and neck. That contamination is trapped within the fabric of the headwear. A small amount may then be released, but that would be miniscule compared to what is released from the rest of each body* in the theatre**. If a sterile gloved hand were to touch a person’s headwear, that would breach the sterile field and immediate regloving should occur. I see addressing the varying level of contamination found on different types of headwear as a distraction from factors more relevant to infection prevention.
*The most prolific site of release is probably the perineum. There have, in the distant past, been suggestions that the surgical team wear tight-fitting rubber underwear to contain such dispersion. This did not seem to find favour with the surgical community.
**The overall level of airborne dispersion in theatre depends on the number of people and their degree of movement. There is a longstanding tradition that the surgical team is both more numerous and more mobile than the patient. The patient contributes minimally to the contamination of theatre air.
Aggie’s perspective: guideline methodologist’s view
From an evidence synthesis perspective, the central issue is not whether contamination can be detected on theatre caps, because it clearly can. The question is what that observation means for patient outcomes.
The first concern is the implicit assumption that contamination equates to infection risk: contamination on caps → contamination of the sterile field → wound contamination → SSI.
What we really care about is SSI; everything else is less directly relevant. This can be thought of as a hierarchy of outcomes: outcomes that are closer to the patient provide more meaningful and direct evidence, while upstream (surrogate) outcomes sit further away from what ultimately matters. As we move further from the outcome of interest, each step introduces additional assumptions about how one finding leads to another. At each step, underlying mechanisms or confounding factors that we may not fully understand can influence the observed relationships, increasing the risk of misinterpreting the true impact. A useful real-world analogy is coconut oil: it has been shown to reduce cholesterol levels, but this does not translate into a reduction in heart attacks. Do we really care if cholesterol is lower if the outcome that matters remains unchanged? Surrogate outcomes are always of uncertain relevance. Where more direct evidence exists, a study measuring a more distal outcome does not materially change the overall understanding of risk. This reflects a familiar principle: correlation does not imply causation. Detecting contamination does not, in itself, demonstrate an increased risk of infection.
There is also a question of biological plausibility and relative contribution. As Peter mentioned, even if small amounts of contamination are released from headwear, the microbiologist perspective highlights that this is likely to be negligible compared to other, more significant sources of microbial dispersion in the operating theatre. Focusing on a minor or uncertain pathway risks diverting attention from interventions with a clearer evidence base.
Another key consideration is how individual studies are interpreted in the context of the wider evidence base. Studies on this topic, examining more direct outcomes (SSIs and contamination of a sterile field), exist. The systematic review of these studies provides a more reliable summary of the available evidence. While the overall evidence on theatre headgear is generally weak, it consistently shows that head coverings, regardless of type, have little or no effect on SSIs. Where differences in contamination of the sterile field are reported, they suggest the same. For the Rituals and Behaviours guidelines, the guideline development group, which included surgeons, microbiologists, and other experts, interpreted this body of evidence as indicating that headgear has minimal direct impact on patient infection risk. Seen in this context, a single study reporting a less direct outcome does not materially change the overall understanding of risk. Interpreted in isolation, however, it risks distorting that understanding, potentially undermining carefully developed guidance and shifting practice in ways that are not supported by the totality of evidence. A more useful approach is to ask whether new evidence meaningfully changes what we already know. In this case, when considered alongside the existing body of evidence, it adds very little. This touches on principles used in formal evidence appraisal frameworks (e.g. GRADE: assessing study design, quality, and directness), but this is a topic that deserves its own post.
Conclusion
Together, these perspectives highlight a recurring challenge in infection prevention and other fields: overinterpreting findings that are biologically interesting but clinically unproven.
The study of theatre cap contamination is not without value. It may help us better understand potential mechanisms of microbial dispersion, including whether and how such contamination could translate into a risk of surgical site infection. It may also prompt further questions. For example, if certain materials retain bacteria more effectively, could similar principles be applied to control microbial shedding from other, more significant sources? However, the study’s relevance to surgical site infections remains uncertain and such findings should be interpreted with caution.
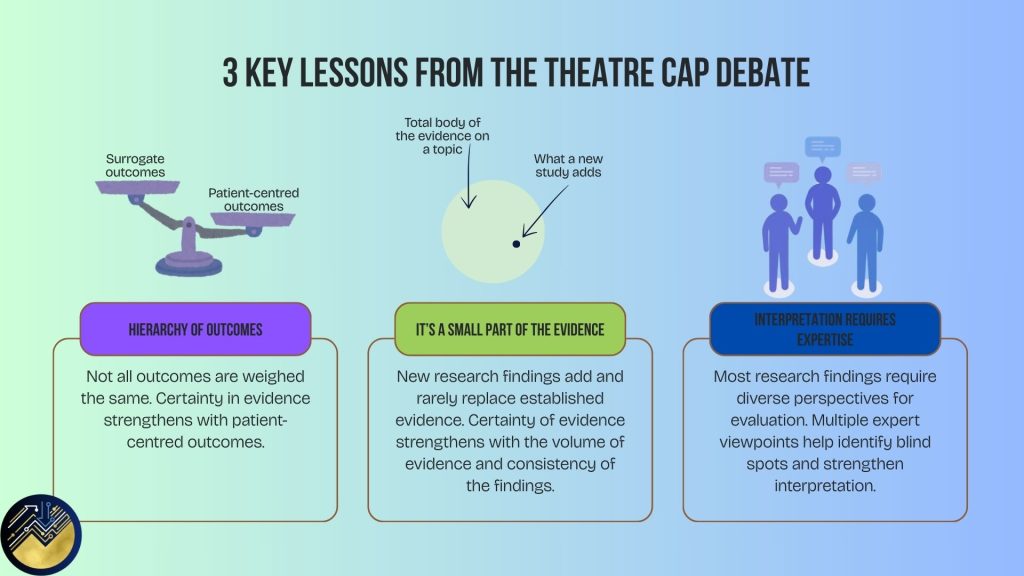
The key lesson is threefold:
1. Changes in distal or surrogate outcomes do not necessarily translate into meaningful clinical benefits.
2. Isolated studies should not be used to overturn the careful, holistic judgements of experts who have evaluated the totality of the evidence.
3. Many studies require interpretation by different types of experts to assess whether the findings meaningfully contribute to clinical practice.